Welcome To Healthysport!
Retirement and Ikigai
- Details
- Written by: Healthysport
- Hits: 1616
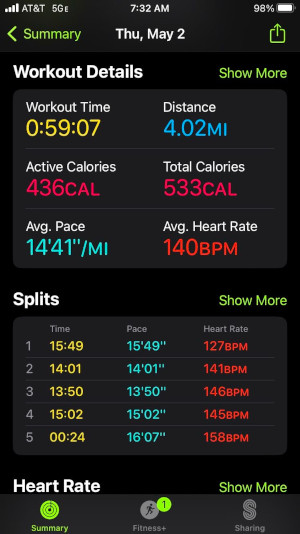
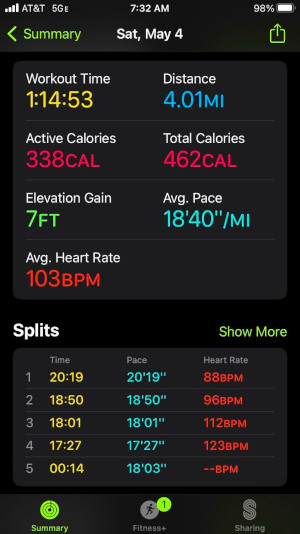
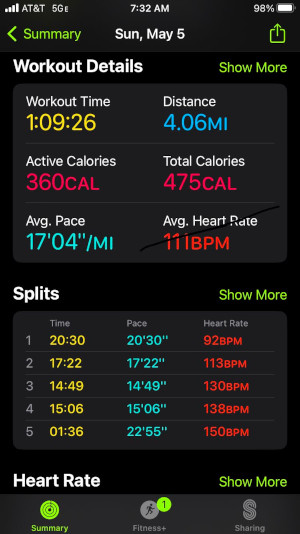
[these are my distances and HR readings in my jogs last week. notice how my heart can reach up to 158 when i increased speed]
I woke up today at around 4 am, lingered on my bed before getting up to meditate. I meditate through written words as I cannot do it mentally (unlike the great meditators who sit quietly and direct their concentration in their minds) as my brain lacks the discipline for that. But writing my thoughts seems to work out. People call it journaling. I usually talk with the Supreme Being about all the things happening around me.
My garden has started to pull my attention again. I find it a little challenging at times, much like my exercises. But it is fulfilling. I surveyed my quarter acre lot to take a mental picture of how to clean and add more color to it. I trimmed the plants that are growing aggressively at the expense of other plants. I am rearranging and modifying their placements. They do respond to my tweaking. I noticed my young jacaranda sprouting new branches after I cut it to size. All the cuttings I started a few weeks ago have sprouted and are replanted and thriving. All is well, I think. But it can be exhausting. All the watering and weeding and replanting can take a lot of your energy.
Another activity I am enjoying is working out. I have avoided the gym since the pandemic, but I am gradually getting back to it. I prefer a very early morning gym workout to avoid the crowd and my sessions are each 1-hour tops. I usually prefer the gym for strengthening, lifting weights, and occasional aerobics, mainly ellipticals and stationary bikes. I would do aerobics in the gym if the weather were bad, but I want my cardio done outdoors all the time. Nothing can beat the fresh wind hitting your face, the sun peeking between the sky clouds, birds twittering and tree canopies dancing alongside me.
[i am back to my favorite leg machines]
I think my right knee is recovering. I am slowly jogging at a more age-appropriate pace. Roughly between 14 to 18 minutes pace, a far cry from the 9 to 10 min pace I used to enjoy as a younger man. There are two things I pay close attention to during my cardiovascular workouts - heart rate and pain. I stay as close as possible to 80 to 90 percent of my maximal heart rate, roughly between 130 -140 beats/minute. I occasionally push my heart a little but not as much as I did when I reached up to 170s heart rate as a young man. One approach I employed to lessen the stress on my knees during my current jogs was to stay on the flat surfaces to run on and shorten the strides.
I will turn 62 in a couple of months and for that, I am preparing myself for what amounts to my new normal. A lot of us imagine retirement as putting an end to work or job as we know it. We imagine staying in bed as long as we want and doing things at a slower pace. But the more I think about it, retirement should be a transition from the usual regular day to day job to another, but this time the new job is easy, light, something we love to do and hopefully can be monetized in the future.
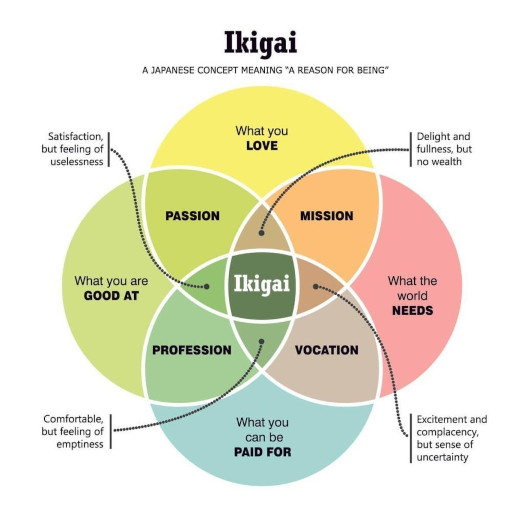
Interestingly, the Japanese have a term for this active retirement. Ikigai.
Ikigai is a Japanese concept that refers to the source of value in one's life or the things that make life worth living. In Japanese, "iki" means "life," and "gai" indicates "worth" or "value." Ikigai is about finding joy, fulfillment, and balance in the daily routine of life, essentially finding one's "reason to live" or "raison d'être." It's a unique approach that combines personal passion, mission, vocation, and profession, leading to a fulfilling life. The concept emphasizes the importance of having a purpose that brings satisfaction and meaning to life (source: Bing definition).
Ikigai also appears related to the concept of flow, as described in the work of Hungarian American psychologist Mihaly Csikszentmihalyi. For Csikszentmihalyi, flow occurs when you are in your “zone,” as they say of high-performing athletes.
Flow is a string of “best moments” or moments when we are at our best. These best moments “usually occur when a person’s body or mind is stretched to its limit, in a voluntary effort to accomplish something difficult and worthwhile” (Csikszentmihalyi, 1990).
Flow can be said to occur when you are consistently doing something you love and that you are good at, with the possible added benefit of bringing value to others’ lives. In such a case, flow might be seen as in tune with your ikigai, or activities that give your life meaning and purpose.
(source: The Philosophy of Ikigai: 3 Examples About Finding Purpose (positivepsychology.com)
The way I see it, I am not embarking on something radical at retirement. My days will still involve workouts, meditating, and maybe a few hours of work here and there. I may include gardening now on days I have more time. My afternoons will be reserved for reading, writing, and programming using different computer languages. All these are my favorite activities with or without pay.
Each retiree has a favorite routine, and mine is unique. Others may want to enjoy time with their family or spend more time with longtime friends. Others would like to travel and perhaps share with the world (social media) their trips. There are others who’d like to focus on spirituality or more learning or even sharing their knowledge through teaching and writing and the latest now is through vlogging. The one thing I’d caution retirees is against investing in businesses they know nothing about. I’ve heard of many sad stories about people who lost a lot of money because they tried and failed in businesses, they thought were easy to manage and earn money but lost everything instead. Remember that when you were young it was easy to fail because you still have all the time to start all over again, a luxury no longer available when old and retired. The best investment a retiree should consider is health improvement. No amount of money can match the ability to wake up one day knowing you can still do what you want to do without limits, or without worrying about the next maintenance pill to make or the next chemo, or the next MD appointment because something needs to be attended to in your body. I’ve also been warned about the boredom of retirement if you didn’t prepare for it, and I am preparing for it. A few people might think that retirement is a complete cessation of work. It should be more like a transition from heavy work to light work, not the other way around. But work, whether paid or not, is still an active lifestyle. I have no idea yet of what kind of work I would pursue. I have an IT degree which I focused on programming in my remote past so that is most likely where I will bury my head into. Someone may suggest that with AI, programmers are now twelve a penny, but I don’t care. There is beauty in figuring things out through mental calisthenics and programming has an edge in that area. I will be doing it to challenge my brain, not to be an expert or an important person.
No one knows the future. Two weeks ago, there was a sudden change in my workplace, and I was ‘forced’ to handle a role that required more responsibilities. I used to be a fast learner but not anymore. Instead of dealing with only two subtasks to an evaluation job I do, I have to add 3 more. This takes time and I am not used to the extra time I now allot to my work on a daily basis. There is a future relief, however, as a new boss to replace the old boss is about to join our team in a week or so. All I need at this point is to hold the fort for a few more months and it will be alright.
Sarcopenia: Loss of Muscle Endurance and Strength
- Details
- Written by: Healthysport
- Hits: 2155

Sarcopenia is the loss of skeletal muscles as we age and this affects our overall strength and performance. This is translated into the inability to perform regular tasks which are necessary for daily living. A person suffering from sarcopenia may need walking aids, would suffer from poor strength of muscles, and start fearing mobility challenges like stairs or stepping on a bathtub; some would be very unsteady on uneven terrains such as rocky backyard to grass lawn to sandy beach because of the risk of imbalance and falls. They resort to the safety of a stable structure like a rail, a tree trunk or someone to hold on. You see them in the airports looking healthy but could hardly walk a certain amount of distance.
Sarcopenia occurs much later in life, most likely after the age of 70. There is a difference between sarcopenia and disability and those who fake weakness LOL. I am often amused by those who can run and jump in real life but suddenly require a scooter in Publix or a wheelchair in airports. If you ask me, I will rather walk as much as I can, even parking far from the entrance of malls, or Walmart or Publix. There is nothing more beautiful than rising up from sitting and taking steps no matter how slow. The ability to move is a gift from God and I don’t know why some would like to immobilize themselves. Some healthy people or those with very minor limitations try desperately to obtain a disabled parking permit. What is the idea? I mean, I can walk 5 miles in one sitting and why would I all of a sudden be so desperate to make a quick zip line to the grocery store? I am not generalizing. I just know some people who are like that. Obviously, there are exemptions. Buying bulky items and furniture would make sense to park closest to the entrances of stores. But ordinary shopping should encourage a healthy lifestyle among people by walking longer in good weather.
Especially when retired with extra time. Why not take the scenic route? I park a safe distance from any store so I can take extra steps.
I live downtown and when the traffic is slow, I walk from my house to the beach. Some people walk their dogs. Some walk back and forth in their gardens. Some walk in parks and chat with friends and strangers and neighbors increasing their networks and sociability. That improves mental health (if that is your thing). Some retirees volunteer in local facilities like hospitals and churches to allow them to frequently sit and stand. There is nothing wrong with greeting and directing people especially if it lifts the spirit and burns calories.
There is a catch though. Mobility like walking is healthy cardiovascular but Sarcopenia weakens muscles also. Conventional wisdom states that as we get older, we need to combine cardiovascular and muscular strength. The strength of the muscles is reduced at a rate of 3% per year after middle age. That is a reduction in volume and mass. It is atrophy but it isn’t demonstrated because what makes up for the lost mass volume is fats. That fat within the muscles reduces metabolism and affects things like speed, endurance and balance.
So it is imperative that a good workout would include cardiovascular training for endurance and muscle training for strength. Both needed to reduce the functional and safety decline in aging.
Then the question is when do you do cardio and when do you do strength? Do you do them separately or at the same time (meaning in the same session). There are studies done on this and they all agree that doing them together in a single session is counterproductive, it seems one cancels the other. In other worlds the buildup of endurance may reduce the buildup of strength. The evidence suggests that endurance one day and strengthening on another day may be the best exercise program to achieve both.
What is endurance? It is the ability to perform light tasks, like walking, cooking, gardening, showering, and light household cleaning for a long time before experiencing tiredness. Strength on the other hand is the amount of effort exerted by the muscles to perform a usually short duration task. Such as lifting an object, standing from sitting, getting out of bed, picking up an object from the ground, countering an abrupt loss of balance, maintaining balance (balance is an interplay of many muscles in the body).
Lean forward (with extra care of course) and you will observe and feel different groups of muscles acting together to correct your lean. Standing on one leg, such as putting on your pants, would suddenly recruit a lot of muscles in the body to maintain your balance. Sit on a therapeutic ball and you would feel the tension in your core as your trunk muscles simultaneously contract to maintain a midline posture. This is a factor one should consider as one ages. If one focuses exclusively on cardiovascular endurance without strengthening, there is a high risk of falling and injury. If one focuses exclusively on strengthening, medical problems such as high blood pressure, high cholesterol, blood sugar etc. may not be addressed.

It goes without saying there are many arguments over this. The strengthening proponents claim that strengthening can be altered to impact the cardiovascular while the cardiovascular proponents claim the same with endurance exercises.
Circuit training is an example of both cardio and strengthening programs. If you advance your endurance exercise up to speed, such as a quick turnover of your legs, carrying weights in both arms, or both legs, running on ramps or elevations, speeding your bicycle up a hill or mountain, stairs are considered both endurance and strengthening exercises. High-Intensity Interval Training that are short spurt but high-impact routine for HIIT such as:
- Burpees
- Mountain Climbers
- Sprints
- Tuck Jumps
- High Knees
- Lateral Lunges with Hops
- Box Jumps
Can be structured to increase strength and endurance if done correctly. But I am getting outside of the Sarcopenia topic here. HIIT may be good, how but I am not sure how many ordinary senior citizens can work this out. It would probably require lots of modifications. A debilitated person might invite more injuries if these HIIT programs are attempted. There are always exceptions, but it might be more prudent to have a professional exercise coach who is familiar with the limitations of old age get you started first.
There are evidence-based studies which also show that combining endurance and strengthening in the same session is counter-productive. Since sarcopenia and old age lessen the mass and strength of muscles, it is important to separate the two goals on separate days. In my case, I do a minimum of three days cardio and two days strengthening per week. I incorporate rest and relaxation on non-workout days.
Resources:
TWENTY-FOUR MONTHS’ RESISTANCE AND ENDURANCE TRAINING IMPROVES MUSCLE SIZE AND PHYSICAL FUNCTIONS BUT NOT MUSCLE QUALITY IN OLDER ADULTS REQUIRING LONG-TERM CARE, A. YOSHIKO, T. KAJI, H. SUGIYAMA, T. KOIKE, Y. OSHIDA , H. AKIMA (authors), Journal of Nutrition, Health and Aging 2019
PHYSICAL ACTIVITY - DECISIVE FACTOR FOR FULL LIFE OF PEOPLE IN AGE, Valentina Vassileva (author), Activities in Physical Education and Sport 2015, Vol. 5, No. 2, pp. 214-217
THE EFFECTS OF UPPER BODY STRENGTH TRAINING VERSUS CONCURRENT STRENGTH + ENDURANCE TRAINING ON INDICES OF STRENGTH, AEROBIC POWER, AND MUSCLE CROSS SECTIONAL AREA, Jose Antonio (author), Nova Southeastern University, Fight Science Lab, Exercise and Sport Science, Davie Florida USA 33328, Journal of Exercise Physiologyonline August 2023 Volume 26 Number 4
- On Bad Blood
- Take Care of Your Heart: A friendly Reminder from the American Physical Therapy Association
- Morning Has Broken
- Reaction to Quiet by Susan Cain
- Stroke Part 5 : The Bleeding Pipe
- Reaction to the book 'The Beginning of Infinity (part 2)
- Book Reaction: The Beginning of Infinity(part1)
- Stroke Part 4: The good, the bad, and the bad (Cholesterol)
- Let's Take a Walk on the Wild Side
- Stroke Part 3: Burst vs Clogged Pipe
Page 29 of 93